

Montana youth aged 11-18 die from suicide at a rate 4.5 times the national average. Suicide is the second-leading cause of death in that age group, and over 25% of the state’s high school students claim to have seriously considered ending their own lives.
Montana’s decades-long mental health epidemic, driven by social isolation, lack of access to care and substance abuse, among other factors, has been widely reported. But new data indicate that, among teens, the crisis may be growing even worse.
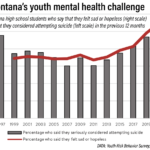
In screenings over the past year by the Rural Behavioral Health Institute (RBHI), over 40% of Montana high school students reported feeling sad or hopeless — a finding that was confirmed empirically when they were unable to continue with usual activities for two or more consecutive weeks due to their emotional state. Only 25% of students reported such behavior in 1999.
That’s why schools and mental health practitioners are ramping up responses. Jefferson County School and Daycare Nurse Erin Ritchie, in partnership with RBHI, is spearheading an initiative in Boulder schools to identify depression and suicidality in students.
This past December, Ritchie, who is also a member of Jefferson County’s Mental Health Local Advisory Council, conducted a digital wellness assessment among 7th and 8th graders at Boulder Elementary. Of the 40 students who opted to participate in the screening, roughly 40% were flagged as needing some mental health intervention.
“We aim to identify suicide risk, and also cases of anxiety and depression,” said Ritchie. Studies have shown that students are more likely to respond honestly to digital wellness questionnaires than in face-to-face screenings. The survey asks students to assess the frequency of which they engage in or are exposed to certain behaviors, such as how many times in the past year they were in a physical fight or if they’ve ever experimented with certain illicit substances.
Students may be screened twice a year to best filter for situational emotional shocks, such as a break up or an isolated family conflict. A ‘high risk’ student is one that has moved beyond suicidal ideation, or thoughts of suicide, to actively preparing to end their own life.
Students identified as ‘high risk’ for suicidality or depression receive a same-day intervention from RBHI’s network of licensed healthcare professionals, via zoom. RBHI employs four full-time therapists, and two part-time.
Once parents are informed, an additional screening takes place and an intervention plan is built. Should that plan involve programs or resources with lengthy waitlists, students can receive up to eight weeks of bridge care, a transitory form of care meant to act as a stop gap while students get connected to longer term resources. This allows high-risk students to immediately enter cognitive behavioral therapy, an evidenced-based psychological treatment meant to help students identify problematic patterns of thinking and behavior.
In addition to the wellness assessment, Ritchie provided students with training, called “Signs of Suicide,” from a wellness consulting firm, Mindwise Innovations. The two-hour-long workshop aims to provide students with the tools they need to identify suicidality and depression among their peers, and to appropriately intervene when someone they care about presents symptomatic behavior.
The program aims to encourage help-seeking behavior through the ACT technique: Acknowledge signs of suicide in a friend, show your friend that you care, and tell a trusted adult. According to Mindwise, students who reported suicidal ideation in the training’s prescreening were 96% less likely to to engage in suicidal behaviors after completing the program.
“Early intervention is key. That’s why when we look at the survey, we approach those flagged as low-risk too. You have to have crisis care, but we want to go way upstream of that and say ‘What can we do before it ever comes to a crisis point?’” said Ritchie.
While early identification can meaningfully impact student health outcomes, Montana faces a shortage of care. According to Kayleigh Brown, RBHI’s Montana-based implementation director, there are only 20 to 30 practicing child psychiatrists in the state, less than one per 100,000 students. Nationally, there are on average 9.75 child psychiatrists available per 100,000 children.
“Everyone deserves help when they’re struggling,” said Brown. “While accessing mental health resources, especially in rural communities, can be difficult, one of the biggest barriers to care is identification. Our network aims to connect students with the resources they need early enough to make a difference.”
From September to date, RBHI has conducted 12,000 screenings in Montana. It hopes to complete 22,000 screenings in the coming year, and to double that number in its 2025 fiscal year. Ritchie herself hopes to conduct the RBHI digital screening and Signs of Suicide training in Jefferson High School this year, and to eventually expand the training to all schools in Jefferson County.
“Yes, there’s the issue of access to care. But there’s also an enduring stigma around reaching out at all,” said Brown. She stressed the importance of parental involvement in addressing mental health concerns, from encouraging their children to pursue care to educating themselves on safeguarding access to common lethal means, such as medication and firearms.
Brown believes that interventions such as those taken by Ritchie are key to improving student mental health. “Erin is an amazing advocate for her community,” said Brown. “With people like her, we can make a real difference.”
If you or someone you know is struggling with thoughts of suicide, call 988 for the National Suicide and Crisis Hotline.


{kind=link}